
Authors


Heart valves are important to keep blood flowing through the heart and around the body. Unfortunately, these valves can become diseased with older age and in younger patients too if they have a condition called congenital heart disease.
Aortic valve disease is the most common type of heart valve problem and can be treated with surgery. However, some surgical procedures to replace aortic valves are not ideal for younger patients, particularly those under 30, as they require patients to take life-long blood thinning medications or have repeat surgery a few years later.
Our specialists are trialling a new type of combined surgical procedure for young and middle-aged adult patients called Ross-PEARS which will ensure a long-lasting, excellent quality of life for these patients, without needing life-long blood thinning medications.
Heart valve disease in young patients
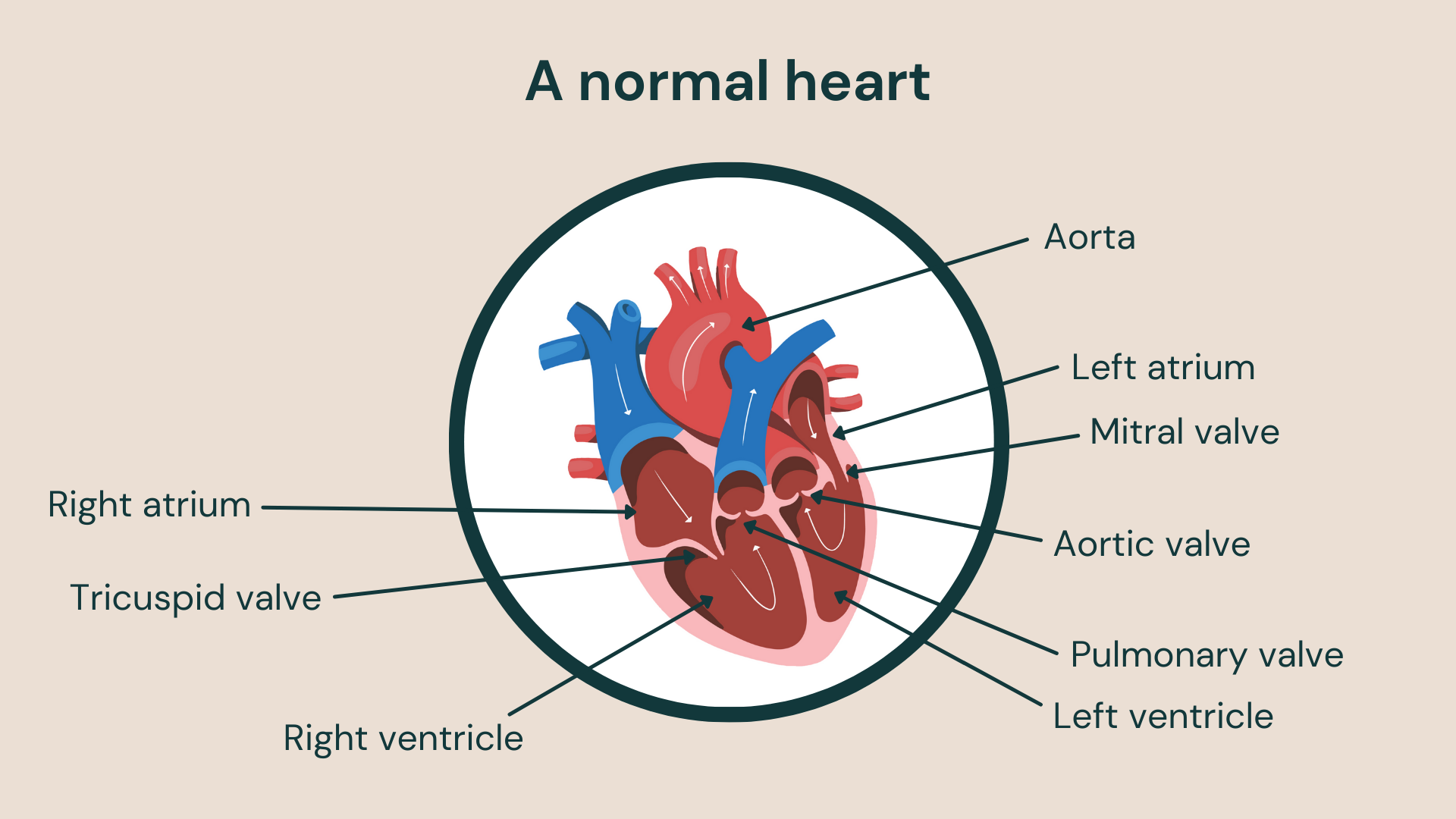
The heart is made up of two lower chambers called the ventricles and two upper chambers called the atria. Every time the heart beats, the muscular walls of the upper and lower chambers contract in turn to push blood through the heart and to the rest of the body to supply organs and tissues with oxygen.
As blood is pumped through the heart, it passes through four heart valves which prevent the backward flow of blood. Unfortunately, these heart valves can become diseased with older age, but also in younger patients too who have a condition called congenital heart disease.
Congenital heart disease is a term used to describe a range of birth defects that disrupt the way the heart normally works and affects up to 1% of new-borns worldwide, making it the most common birth defect. The heart muscle walls, valves and arteries and veins near the heart can all be affected.
The condition is normally diagnosed during pregnancy but can be discovered after birth or years later in childhood. Treatment depends on the type of heart defect but people with congenital heart disease often need monitoring and treatment throughout their lives. For example, they may need heart valve surgery in their 20s or 30s.
Replacing a faulty aortic valve
Aortic valve disease is a condition where the heart valve between the aorta (which is the main artery of the body) and the left ventricle (which is the chamber that pumps blood out of the heart) becomes faulty. Like other heart valve diseases, it can occur in younger patients due to congenital heart disease.
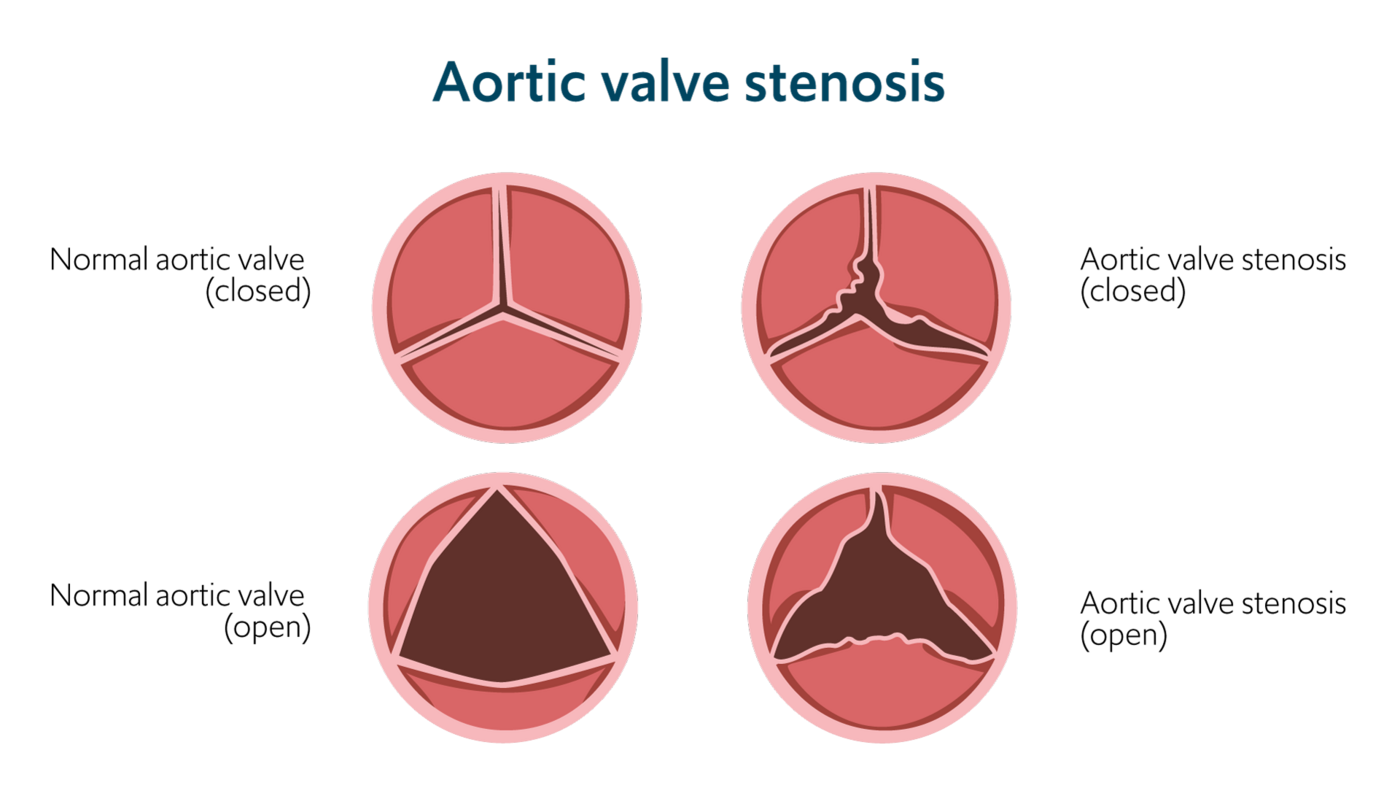
The aortic valve opening can become narrowed due to its leaflets (also known as flaps) becoming thick and stiff. This is called aortic valve stenosis and can reduce or block blood flowing through the heart. The valve can also become leaky if it doesn’t close properly, causing blood to flow backwards in the heart – this is called aortic valve regurgitation.
Aortic valve replacement is the most common form of heart valve surgery and is used to correct both aortic stenosis and regurgitation. However, the choice of procedure in young and middle-aged adult patients is challenging as it needs to provide long-term results to prevent the need for repeat surgeries in future as well as enabling a physically active lifestyle and avoiding the need to take blood thinning medications.
The most common type of aortic valve replacement used is called a mechanical valve. These valves are made of hard-wearing synthetic materials which make them very durable, but they can cause blood clots and so require patients to take blood thinning medications for life. This exposes them to a range of complications such as a stroke.
There is another type of valve which is called a biological valve that is made of animal tissue and is the most suitable for younger patients, particularly those under 30, as they don’t require patients to take blood thinning medications. However, they can deteriorate and require repeat surgery within a few years.
A better approach for replacing aortic valves in younger patients
The Ross procedure is an alternative way of replacing the aortic valve in young and middle-aged patients with a biological valve. Rather than a biological valve made from animal tissue, it utilises a patient’s own healthy heart valve and one from a human donor.
The pulmonary valve, is similar in structure to the aortic valve but unlike the aortic valve which is under high pressure with blood flowing to the entire body, is under lower pressure as blood only flows to the lungs. Due to the difference in blood pressure flowing through it, the pulmonary valve is usually healthy in patients even if the aortic valve is faulty.
The Ross procedure utilises the biological similarities between the two heart valves to replace the diseased aortic heart valve with the patient’s own healthy pulmonary valve. The pulmonary valve is then replaced with a healthy valve from a donor which is cryopreserved (preserved through freezing) until it is needed.
Once implanted, the pulmonary valve goes through a process called adaptive remodelling, meaning it can closely mimic the function of the aortic valve it replaced. Studies have shown that, following the Ross procedure, the heart valves closely mirror the function of normal healthy heart valves even during strenuous physical exercise. Also, as human valves are used, patients don’t need to take blood thinning medications.
A recent long-term study of the outcomes of the ROSS procedure on 414 patients over 18 years demonstrated a long-term survival rate of 89.3% at 15 years. This survival rate was similar to people in the normal population of the same age and gender. There was also a low number of repeat surgeries needed. Patients can therefore expect long-lasting results with an excellent quality of life.
As the Ross procedure is complex, it is most safely performed at an experienced centre. Surgeons at our specialist hospitals have been performing the Ross procedure for over 30 years with favourable results.
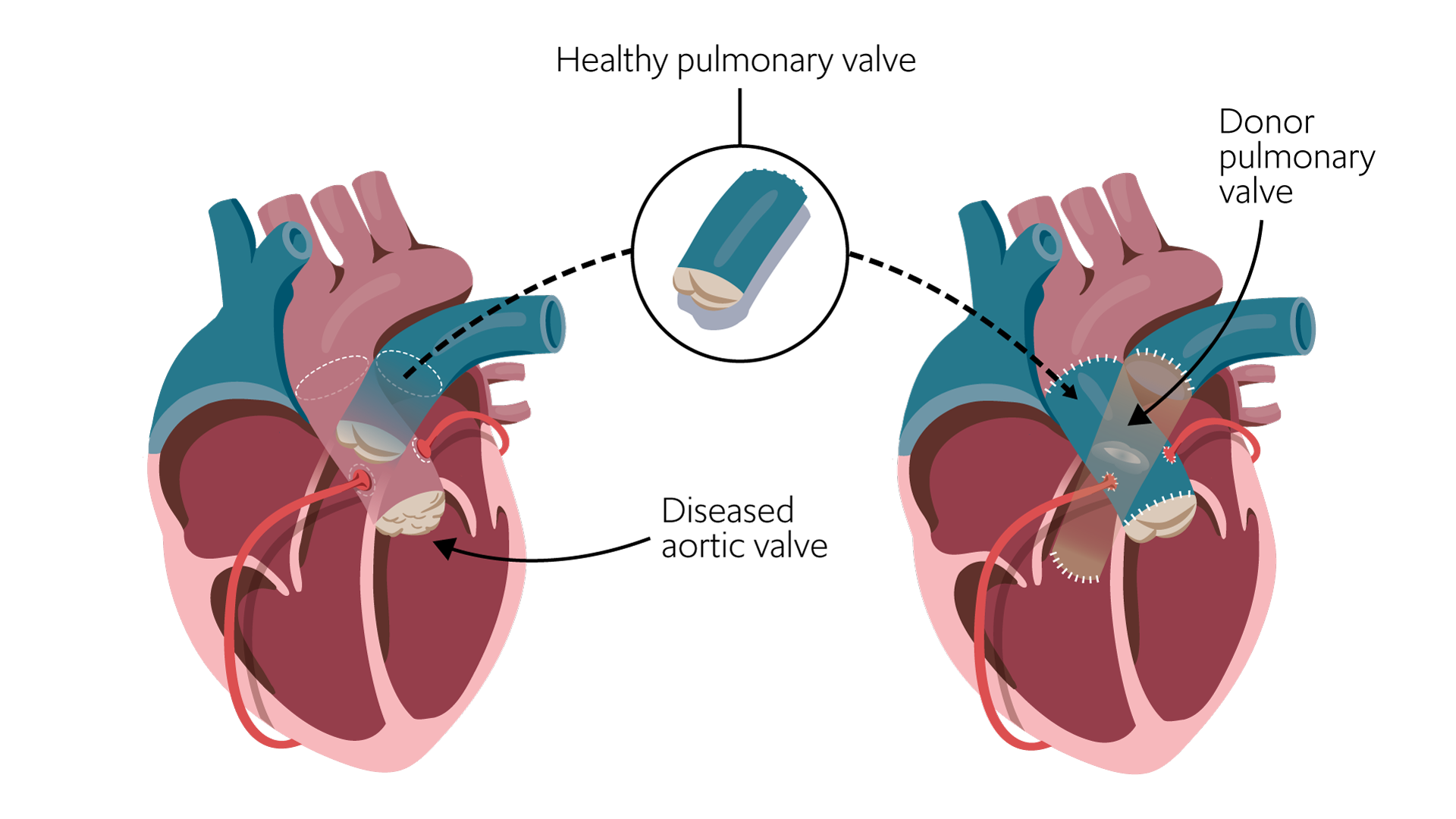
The Ross procedure: The diseased aortic valve is removed and replaced with the patient’s own healthy pulmonary valve – called a pulmonary valve autograft. The patient’s pulmonary valve is then replaced with a cryopreserved donor pulmonary valve.
Our experts are working to improve the Ross procedure
Although patients can expect excellent long-term results with the Ross procedure, the pulmonary valve which is used to replace the diseased aortic valve (called a pulmonary valve autograft) can itself require replacing 15 years later in 10% of patients.
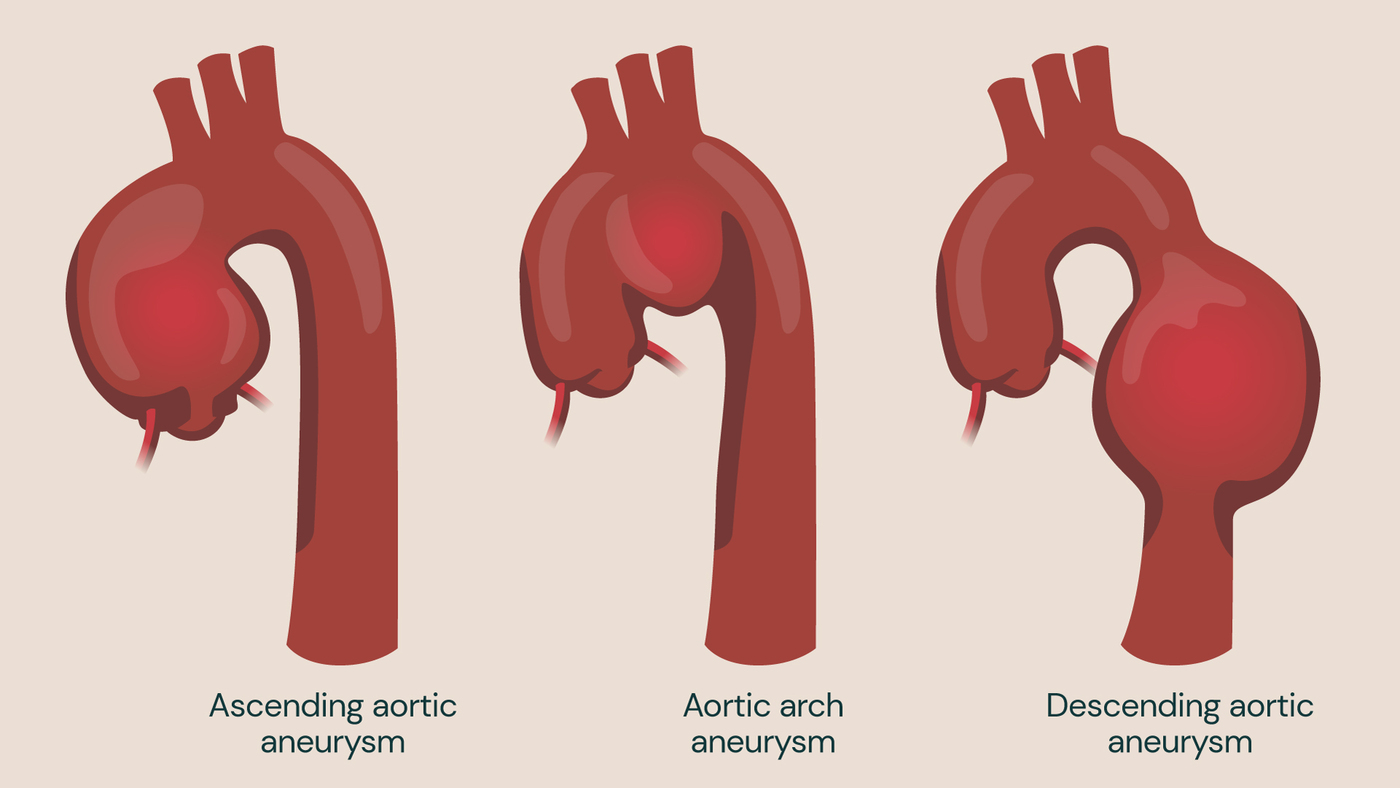
This may happen due to a condition called aortic root dilation (also known as ascending aortic aneurysm), where the base of the aorta – the largest artery of the body – expands at the point where it meets the heart and where the aortic valve is located. This puts strain on the pulmonary valve autograft causing it to become damaged over time.
Surgery to reinforce the aorta at its base – the root – with a synthetic support following the Ross procedure has been shown to reduce the need for reoperation on the pulmonary valve autograft.
Personalised external aortic root support (PEARS) is a relatively new aortic root reinforcement system. It was originally developed at our hospitals for patients with Marfan syndrome – an inherited condition affecting the body’s connective tissues which causes patients to experience aortic root dilation at a young age.
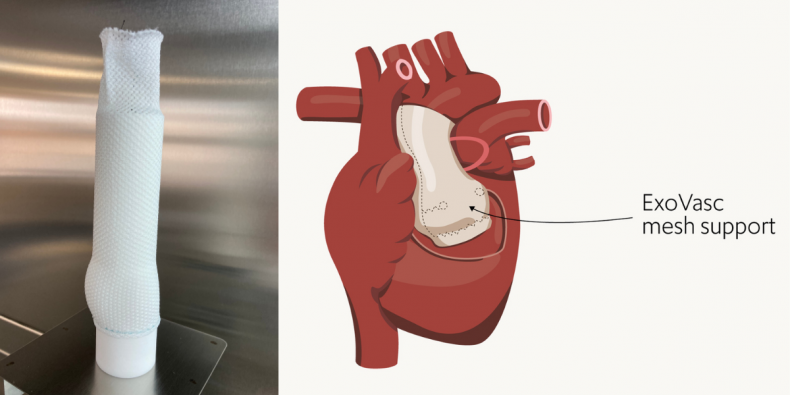
The PEARS procedure: (L) the ExoVasc mesh support formed on an anatomically precise model of the patient’s aorta and (R) a visual of the mesh support implanted around the patient’s aortic root.
With the PEARS procedure, a synthetic ExoVasc polymer mesh sleeve is used to support the aorta and aortic valve to prevent them from expanding. Advanced medical imaging and computer-assisted 3D printing is used to create a precise model of the patient’s aorta that is personalised to the unique anatomy of the patient. This model is then used to form the textile ExoVasc implant. The ExoVasc textile implant created has 0.7mm pores which enable the patient’s cells to enter and adhere it firmly to the patient’s tissues for greater long-term durability.
“The PEARS procedure has been successfully performed on over four hundred patients with Marfan syndrome worldwide. However, its use in the Ross operation is fairly new,” explains our consultant cardiac surgeon, Professor John Pepper, who pioneered the PEARS procedure at Royal Brompton Hospital and advises our consultants on the PEARS, Ross and combined Ross-PEARS procedures.
“By adding aortic root reinforcement with PEARS to the Ross procedure, we hope to reduce the number of patients requiring reoperation on the pulmonary valve autograft. For young and middle-aged adult patients, we want to make sure that any treatment offered enables them to live for as many years without re-intervention as possible, with an excellent quality of life.”
In the Ross-PEARS procedure, it is the pulmonary valve autograft that is modelled and an ExoVasc implant produced to support it when it is re-implanted to replace the aortic valve.
Our consultants are leading experts in the combined Ross-PEARS procedure, with over 40 procedures performed so far across our hospitals and our consultant cardiac surgeons, Mr Jullien Gaer, Mr J Andreas Hoschtitzky, Mr Mario Petrou and Professor Darryl Shore all perform it at our centre.
Mr Conal Austin, consultant cardiothoracic surgeon at Guy’s and St Thomas’ NHS Foundation Trust – which we have recently merged with, also performs the Ross, PEARS and combined Ross-PEARS procedure, but does not currently operate at Royal Brompton and Harefield hospitals.
Helping Fabio get active again

Fabio was treated by Mr Hoschtitzky with the Ross-PEARS procedure
Fabio was used to keeping a close eye on his heart from a young age. This is because he was born with a ventricular septal defect also known as a ‘hole in the heart’.
This is one of the most common birth defects of the heart (medically termed ‘congenital heart disease’) and makes it harder to pump blood around the body.
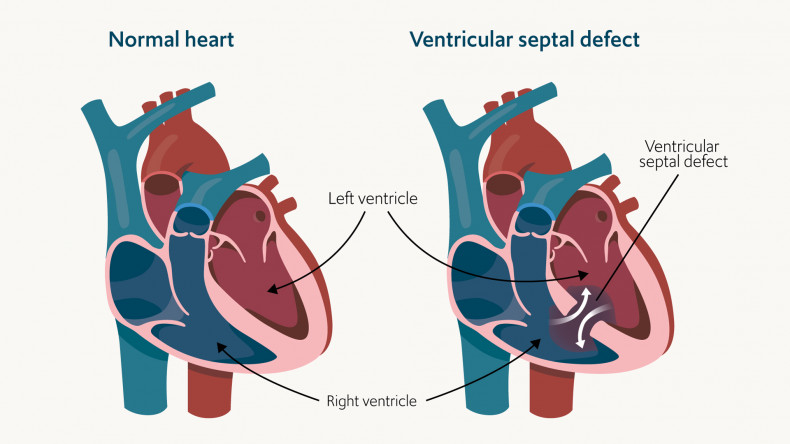
A ventricular septal defect is an example of congenital heart disease, where a hole appears between the lower chambers of the heart, called ventricles. This causes blood to be pumped into the lungs rather than the rest of the body as it normally should.
To resolve his heart problem, doctors in Italy (where he was born) performed corrective heart surgery at the age of 15.
“My doctors managed to fix my heart and I lived a relatively normal life with routine heart checks,” says Fabio.
“I worked for many years in the cruise industry which was physically demanding, but I enjoyed staying active and got to see the world.”
In 2014, he moved to the UK where he was referred to the care of our consultants at Royal Brompton Hospital to continue his routine heart checks and remained fit and healthy.
Encouraged by his partner, he took up Tai Chi and yoga, which he practiced for over five years. He explains: “When you’re born with a heart condition, you become very conscious of your health and I have always tried to stay fit and healthy.”
However, in 2019 at the age of 39, he noticed his heart health start to deteriorate gradually.
“I started to experience heart palpitations and feeling faint and dizzy. At first, this happened once every couple of months, but this became multiple times a week,” Fabio explains.
Unfortunately, his symptoms caused him to stop driving, cycling, and taking part in the activities he loved.
Our consultants assessed Fabio’s heart and found his aortic valve was faulty, causing him to experience the symptoms he felt. This is when he was referred to the care of Mr Hoschtitzky for assessment for the Ross-PEARS procedure to replace his aortic valve.
“Mr Hoschtitzky talked me through my treatment options and the Ross-PEARS procedure was a no brainer. I didn’t want to be on blood thinners for the rest of my life and I would get to keep my own heart valve,” he says.
In October 2020, Mr Hoschtitzky successfully performed the Ross-PEARS procedure on Fabio, and he is now on a steady path to recovery – he has even started jogging again.
“It’s crazy to think that I was on a surgical bed and feeling really unwell two months ago and now I’m jogging. I know I still have a journey ahead in my recovery and getting back into the more intense sports I enjoyed but it’s going great so far,” he explains.
“I only have extremely nice words for everyone at Royal Brompton Hospital – from the nurses to the consultants. They looked after me really well and I feel very fortunate to have had a procedure that isn’t widely available.”
Get in touch
For more information or to book an appointment, please contact our customer care team.
Reviewed regularly to reflect clinical best practice
Last reviewed: 11 November 2025
Related content
-
Aortic stenosis
Aortic stenosis is a disease that affects the main outlet valve of the heart and is the third most common cardiovascular disease.
-
Personalised external aortic root support (PEARS)
Personalised external aortic root support treats and manages aortic dilation and dissection in patients with Marfan syndrome.
-
Heart valve repair or replacement
Heart valve surgery can repair or replace a damaged valve.