
Authors

Tricuspid regurgitation becomes increasingly common in those over 65, but corrective open-heart surgery is often considered too high-risk to perform in older patients. A new minimally invasive transcatheter approach is now available at our centre that enables us to target treatment directly to where it is needed and offer significant improvements to quality of life in patients where surgery is not possible.
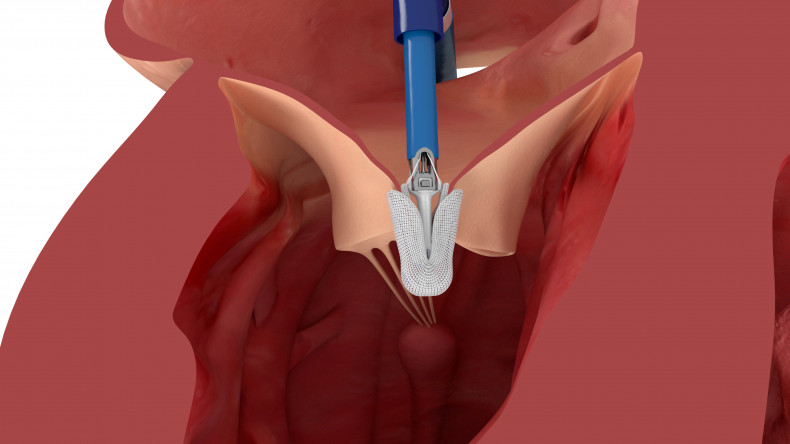
The Edwards PASCAL transcatheter valve repair system with the PASCAL Ace implant.
The burden of tricuspid regurgitation
Tricuspid regurgitation (TR) occurs when the tricuspid valve does not close sufficiently, allowing blood to flow backwards from the right ventricle into the right atrium.
This places substantial strain on the heart as it must work harder to pump blood forward towards the lungs. With time, this can lower cardiac output and places patients at increased risk of right-sided heart failure.
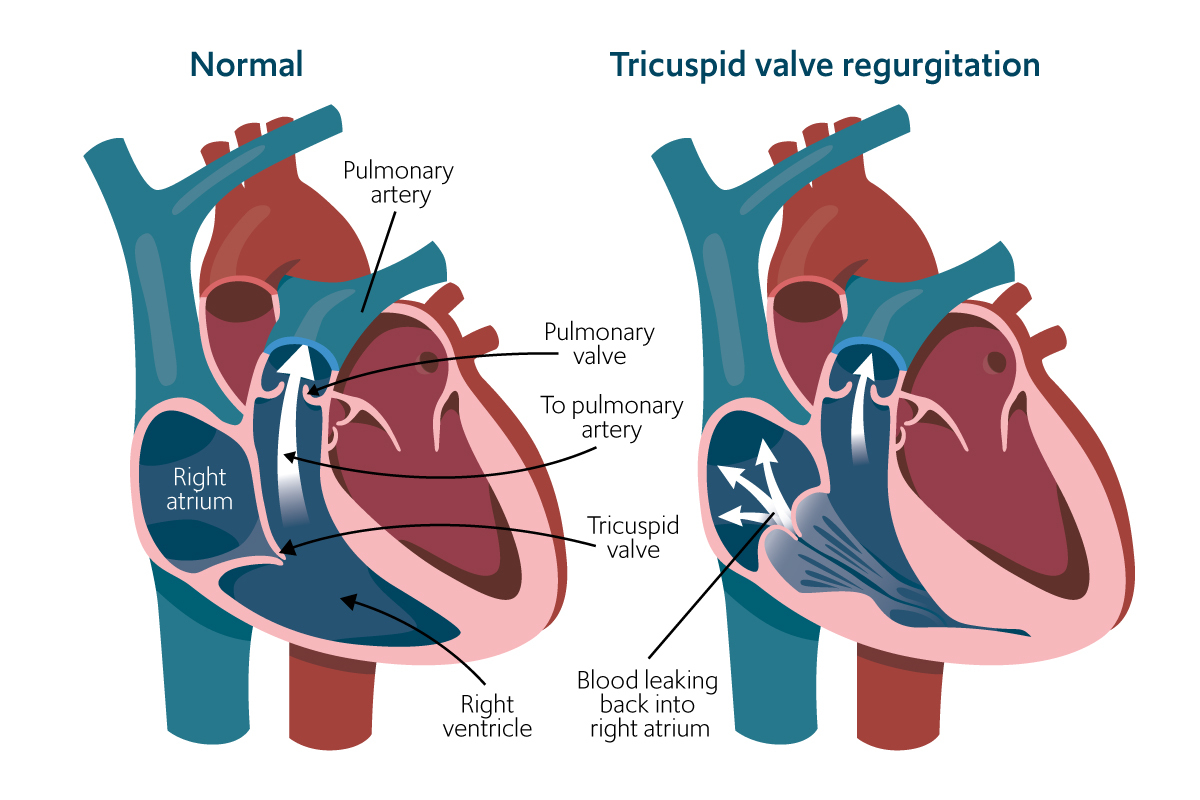
Tricuspid regurgitation: The heart works harder to push blood forward.
TR can result from a range of factors. This can include wear and tear due to age, enlargement of the right atrium due to atrial fibrillation, congenital heart disease, rheumatic disease, and structural damage from cardiac device implantation.
The most common form of TR is termed secondary (or functional). Secondary TR affects 80-90% of patients and is caused by changes to the right ventricle or distortion of the tricuspid valve leaflets, annulus, or chords. This typically occurs in patients with left-sided heart disease, pulmonary hypertension, atrial fibrillation or right ventricle dysfunction.
Generally, patients are classified as having mild, moderate, or severe TR and the overall prevalence varies widely in Europe, with figures ranging from 17%-66% (for all forms combined).
TR severity is associated with age and gender – the prevalence of moderate to severe TR rises from 1.1% in those aged 65 and over, to 4% in those aged 75 and over, with women having TR of greater severity when compared with men.
Symptoms and treatment options
During the early stages of TR, the condition is normally clinically silent. As such, TR is often an incidental finding during routine patient examinations, such as during echocardiography.
In the OxVALVE study in people aged 65 and over and diagnosed with valvular heart disease, 97.4% of patients with TR did not experience symptoms.
When symptoms are present, they can include fatigue, reduced ability to exercise, shortness of breath, dizziness, fainting, swelling of the legs or abdomen, atrial fibrillation, and/or kidney disease.
Survival rates decrease significantly with increasing TR severity, with available studies showing survival is approximately 26% at 15 years for those with moderate to severe TR.
Treatment options for medical management of TR are unfortunately limited and may not address the underlying pathology of the condition.
Corrective surgery is usually recommended in both symptomatic and asymptomatic patients with progressive right ventricular dilation and/or dysfunction. Despite this, however, open-heart tricuspid valve surgery is high risk for certain patient groups where it is associated with poor outcomes or mortality.
These high-risk patient groups include those that are older, have comorbidities and/or have advanced heart failure. An alternative, minimally invasive approach is therefore favourable for these patients.
A new minimally invasive approach
We now offer a transcatheter based approach to treating TR in patients where open-heart surgery is not possible.
To ensure that we can provide treatment that is unique to each patient and their tricuspid anatomy, our cardiology experts utilise two different clip-based platforms – the Abbott TriClipTM Transcatheter Tricuspid Valve Repair system and the Edwards PASCAL trancatheter repair system together with the PASCAL Ace implant system.
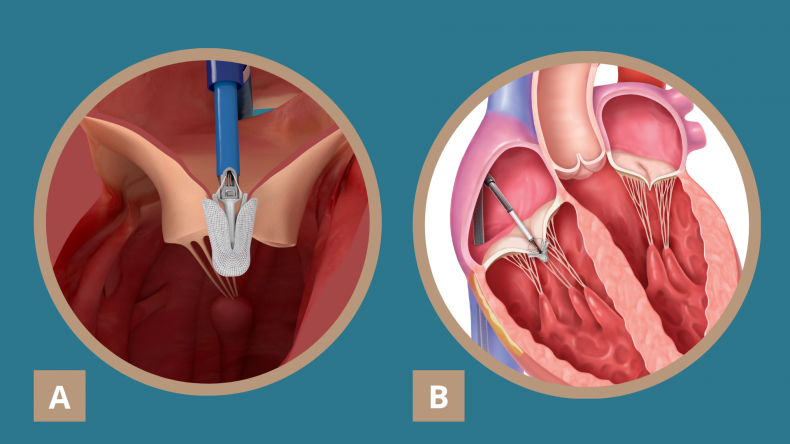
Caption: (A) The Edwards PASCAL trancatheter valve repair system, with the PASCAL Ace implant and (B) the Abbott TriClip Transcatheter Tricuspid Valve Repair system offer our cardiologists a wide range of implants for different tricuspid anatomies to ensure we can provide treatment uniquely tailored to each patient.
Both platforms enable our cardiologists to transeptally deliver the implant via a very small incision in the groin directly to the tricuspid valve leaflets without needing to stop the heart. This minimises the risk to the patient when compared to open heart surgery.
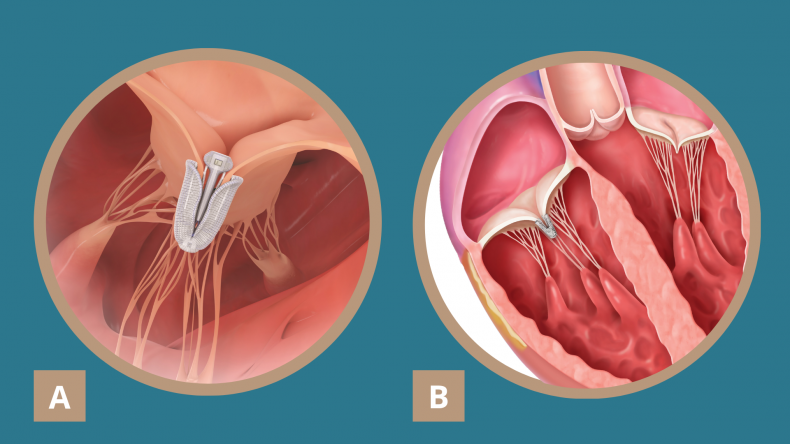
(A) The Edwards PASCAL ACE implant and (B) Edwards PASCAL ACE implant holding the diseased tricuspid leaflets together to reduce tricuspid regurgitation.
“Studies have shown excellent safety profiles for both platforms, with durable reductions in tricuspid regurgitation and improved quality of life for patients,” explains our consultant interventional cardiologist, Dr Rob Smith, who performs this new specialist procedure at our centre.
“We have seen impressive results in our patients who had no alternative surgical treatment option and hope to offer the procedure to more patients who are in a similar situation and may benefit.”
Patients can expect to return home on the next or a couple of days after the procedure and most patients return to their regular routines shortly after.
Our centre is currently one of the few in the world that can offer this innovative new procedure and adds to our extensive expertise in minimally invasive heart valve repair, including the transcatheter edge-to-edge repair procedure to treat mitral regurgitation.
For more information or to book an appointment, please contact our customer care team.
Related content
-
Tricuspid regurgitation
Tricuspid regurgitation is when the tricuspid valve of the heart doesn't close properly.
-
Heart valve repair or replacement
Heart valve surgery can repair or replace a damaged valve.
-
Valvular heart disease
Heart valve disease occurs when the valves of the heart become diseased or damaged.