
Content verified by

Lung cancer is one of the most common cancers in the UK. It typically causes no symptoms in its early stages, but as lung cancer progresses, it may lead to a persistent cough, recurrent chest infections, fatigue and other symptoms.
There are a range of effective treatments for lung cancer, including minimally invasive tumour ablation which kills cancer cells using hot or freezing temperatures applied directly to the cancer. For larger tumours, single-port video-assisted thoracoscopic surgery (VATS) or robotic-assisted thoracic surgery (RATS) may be recommended.
Our world-leading lung cancer specialists at Royal Brompton and Harefield hospitals are internationally renowned. They are pioneers in their field, developing new techniques to diagnose lung cancer earlier and reduce the length of hospital stays following procedures. Some of our patients have returned home on the same day as their lung surgeries.
Experts in lung cancer
Our world-leading consultants offer:
- fast, accurate diagnosis with advanced investigations, including Ion robotic-assisted biopsies
- minimally-invasive treatments, including tumour ablation and single-port VATS
- short-notice appointments, available in as little as 24 hours

What is lung cancer?
Around 48,000 people are diagnosed with lung cancer each year in the UK, accounting for around 13% of all new cancer cases.
Cancers of the lung can originate in the lungs or can spread to the lungs from another part of the body. The former is known as primary lung cancer, while the latter is called secondary lung cancer. This page will focus on primary lung cancer.
Like all other types of cancer, lung cancer happens when certain cells can no longer be controlled by your body and start to change and become abnormal. The number of abnormal cells starts to increase and multiply out of control.
Over time, these can form a lump called a tumour. However, it is also possible for cancerous cells to be present in your body and not cause a noticeable tumour.
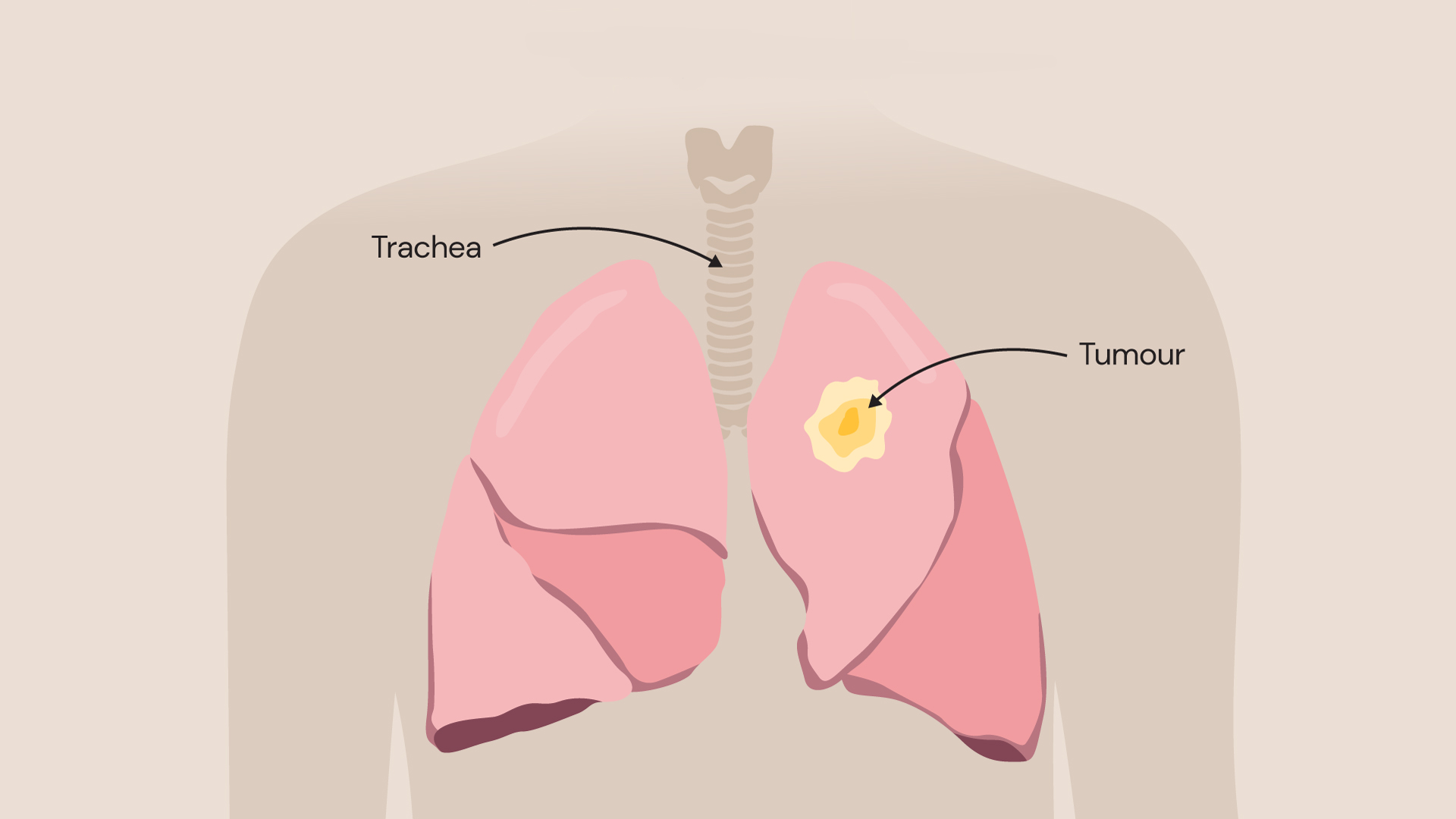
Depiction of a cancerous tumour in the lung
Unfortunately, lung cancer is also one of the most common causes of cancer death in the UK, with around 95 people dying every day from the disease. However, lung cancer mortality rates are predicted to fall over the coming years as earlier diagnoses and new treatments improve patient outcomes.
To learn more about lung cancer treatments available with our expert consultants, contact our team.
Types of lung cancer
There are 2 main types of primary lung cancer. Each type is determined by the type of cell that the cancer first started growing in.
Non-small cell lung cancer
This is the most common form of primary lung cancer, being diagnosed in around 80-85% of cases. There are 3 different types of non-small-cell lung cancer:
- Squamous cell carcinoma: This usually begins in the passages that bring air into the lungs. It also grows more slowly than other types of lung cancer.
- Adenocarcinoma: This is the most common type of non-small cell lung cancer and starts in the glands that line your airways.
- Large-cell carcinoma: This type can appear in any part of the lung and tends to grow and spread quickly.
Small-cell lung cancer
A much rarer form of primary lung cancer, small-cell lung cancer is usually more aggressive and spreads faster.
What causes lung cancer?
Unlike some other cancers, there are several things that are known to make you more likely to develop lung cancer.
It is well-known that smoking cigarettes is the biggest cause of lung cancer and is estimated to account for up to 90% of cases. Other tobacco products are not safe either, with pipe tobacco (shisha/hookah) or even second-hand smoke increasing the likelihood that you will develop lung cancer. The more you smoke and the longer you smoke, the greater your risk.
However, that does not mean it is too late to quit. Studies show that quitting smoking, even after smoking for many years, could still drastically reduce your chances of developing lung cancer in the future.
Other risk factors for lung cancer include:
- a family history of lung cancer
- exposure to asbestos and other air pollutants like diesel exhaust fumes and silica
- exposure to radon gas
- poor immune system caused by conditions like HIV and AIDS, or immunosuppressant drugs taken following organ transplant
- previous radiation therapy
Lung cancer is strongly linked to age with disease rates increasing sharply after 45.
Lung cancer symptoms
There are not usually any signs of lung cancer in the initial stages of the condition. However, as the cancer progresses, you may start to develop symptoms including:
- aching or pain when breathing or coughing
- a persistent cough
- chest or shoulder pain
- coughing up blood
- ongoing chest infections
- persistent breathlessness
- unexplained tiredness
- unexplained weight loss
If you notice any of these symptoms, contact our team to make an appointment with one of our lung cancer specialists.
Lung cancer diagnosis
Royal Brompton and Harefield hospitals are world-leading centres for heart and lung care. We diagnose and treat hundreds of patients with lung cancer each year, with many coming from abroad just to see our consultants privately.
We have internationally renowned experts in imaging and histopathology who can diagnose the type, location, and stage of lung cancer with the greatest precision. This helps guide procedures to remove lung cancer while avoiding harming healthy lung tissues.

A PET-CT scan shows the position of active cancer cells and helps our lung care specialists decide which course of treatment is best.
How is lung cancer diagnosed?
Any lung cancer diagnosis starts with a consultation where you will discuss your symptoms and concerns with your chosen consultant.
You will be asked about your lifestyle and your medical history so that we can build a picture of your day-to-day life. You may also be asked to breathe into a device called a spirometer which measures how much air you breathe in and out.
If our specialists suspect you may have lung cancer, you will be referred for several tests to determine if you have it, and if you do, what type you have and if it has spread. These tests may include:
- a blood test to rule out infections or other causes of your symptoms
- a chest x-ray which will provide a picture of what is happening inside your lungs, enabling us to detect any masses which may or may not be cancerous
- a CT scan – usually performed following a chest x-ray, a CT scan provides a detailed image of your lungs so that any abnormalities can be seen more clearly
- a PET-CT scan – a different type of imaging test which may be done if your CT scan suggests that you have cancer. A PET-CT scan shows the position of active cells and helps your respiratory consultant decide which investigations/treatments would be best for you
- a lung biopsy – a procedure used to take a small sample of tissue, which can then be looked at under a microscope to get more information about the cells, including if they are cancerous and if they are, the type and stage cancer you have
If you need a biopsy, this may be carried out in a few different ways. You may have:
- a bronchoscopy (in which a thin tube is inserted through the mouth or the nose). Our experts use the latest Ion robot-assisted lung cancer biopsy technology to sample tumours when they are still very small in size for a better chance of treatment success
- percutaneous needle biopsy (where a needle is placed directly through the skin into the lungs)
- thoracoscopy or mediastinoscopy (in which tubes with cameras are inserted into the chest through surgical incisions).
Our biopsy service offers outcomes that are superior to the British Thoracic Society standard. In 2019-2021 (our last service audit), we demonstrated 0% 30-day mortality (no deaths from the procedure), 100% diagnostic accuracy and 94% same-day discharge (most patients did not have to stay in hospital after the procedure).
Your lung care specialist will explain which tests you need and what you can expect to happen next. Contact us to book a consultation with our team at Royal Brompton and Harefield hospitals.
Lung cancer risk assessment service
Unfortunately, lung cancer is difficult to treat when it is diagnosed at an advanced stage, with only 1 in 5 people surviving. It is therefore important that the disease is captured in its earliest stages for the greatest chance of treatment success.
Our lung cancer risk assessment service is available for people that are at an increased risk of developing the condition, offering them a chance to be comprehensively reviewed by one of our respiratory consultants.
Our consultant thoracic surgeon, Professor Eric Lim, explains the importance of early lung cancer diagnosis.
People that are at an increased risk of developing lung cancer include those who:
- are over 50 years of age (8 in 10 cases of lung cancer occur in people over 60, but it can occur at younger ages too)
- have a strong family history of lung cancer
- regularly smoke or have a history of heavy smoking
Our specialists will assess your risk of lung cancer during a consultation and recommend further testing if necessary.
Get in touch with our customer care team if you are concerned about lung cancer and would like to book an appointment with one of our consultants.
How is lung cancer treated?
Our respiratory consultants at Royal Brompton and Harefield hospitals are experts in lung cancer care. They are pioneers in minimally invasive lung cancer surgical and non-surgical procedures and are internationally renowned in this field.
We work closely with cancer specialists at Royal Marsden Hospital in London, a world-renowned cancer centre, and Mount Vernon Cancer Centre in Northwood. Consultants at both hospitals provide expertise in chemotherapy, radiotherapy, and immunotherapy, while our specialists provide surgical and non-surgical procedures for lung cancer.
The treatment recommended for your lung cancer will depend on the type you have; how large the cancer is and how far it has spread. Explore our lung cancer treatments below.
Lung tumour ablation
Lung tumour ablation is a minimally invasive technique that avoids the need for surgery. It uses either hot or freezing temperatures applied directly to the tumour to kill the cancer cells, while avoiding harm to surrounding healthy lung tissues.
Tumour ablation may be recommended if:
- surgery is not an option for you
- there are only a few small tumours in your lungs (both primary and secondary tumours can be treated using this method)
- the tumour is in a location in the lungs where it is difficult to operate
Endobronchial tumour ablation (endobronchial cryotherapy)
If the lung tumour is in the airways, a procedure called endobronchial cryotherapy may be performed where a bronchoscope (a tube-like device with a camera at its end) is used to reach it.
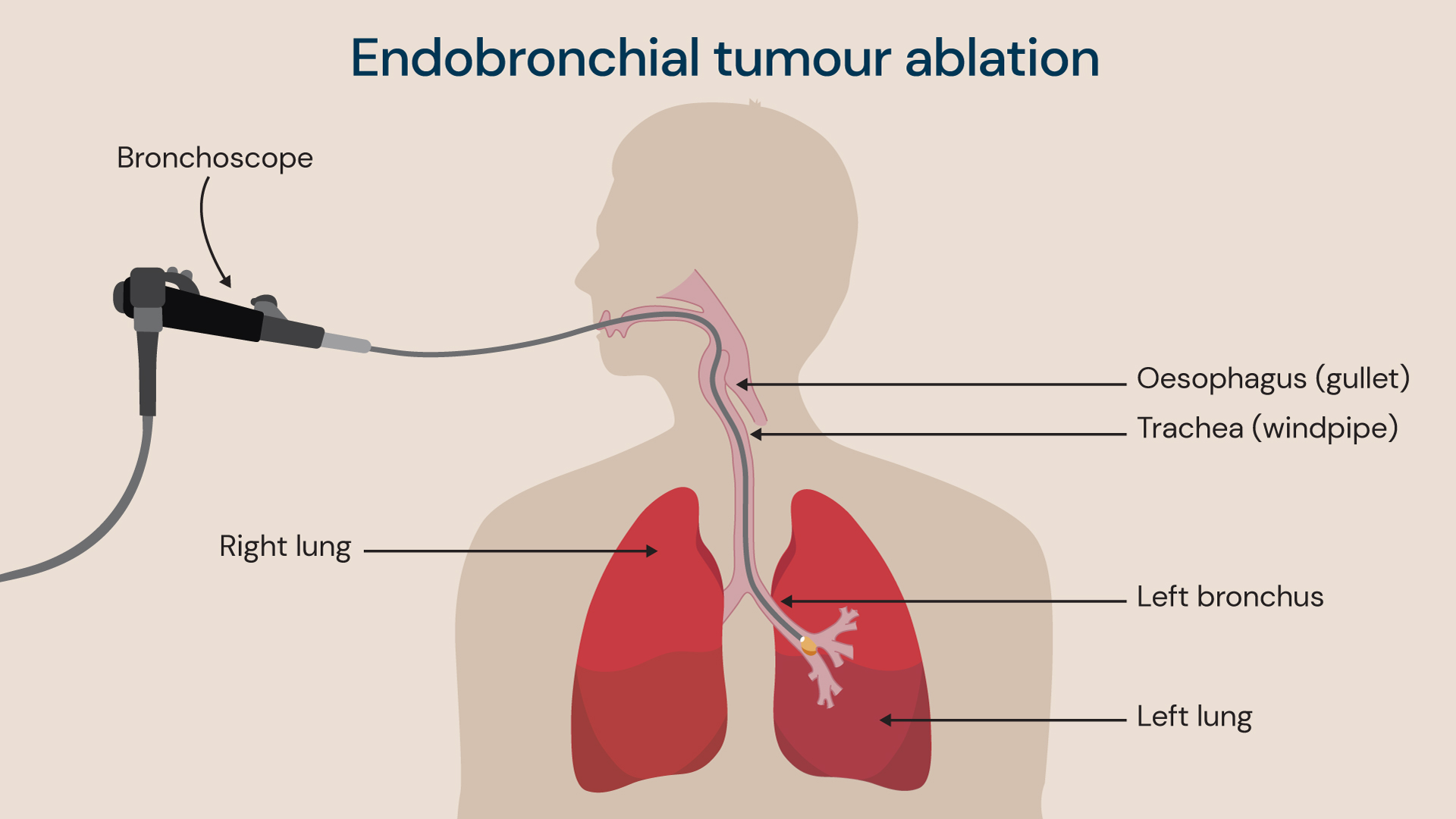
A bronchoscope is used to reach the lung tumour in the airways, before applying very cold temperatures to freeze and kill it.
Our consultants apply a cryogen (a substance that produces very cold temperatures between -78C and -187C) from the tip of the bronchoscope to freeze and kill the cancer cells.
This procedure takes approximately 20 minutes to complete, and you are sedated with general anaesthetic.
Percutaneous tumour ablation
Percutaneous means ‘through the skin’. Our consultants use an innovative ‘pinhole’ technique for our percutaneous tumour ablation procedures where a needle-like probe is inserted into the lungs via the skin and is guided to the site of the tumour with medical imaging to deliver treatment.
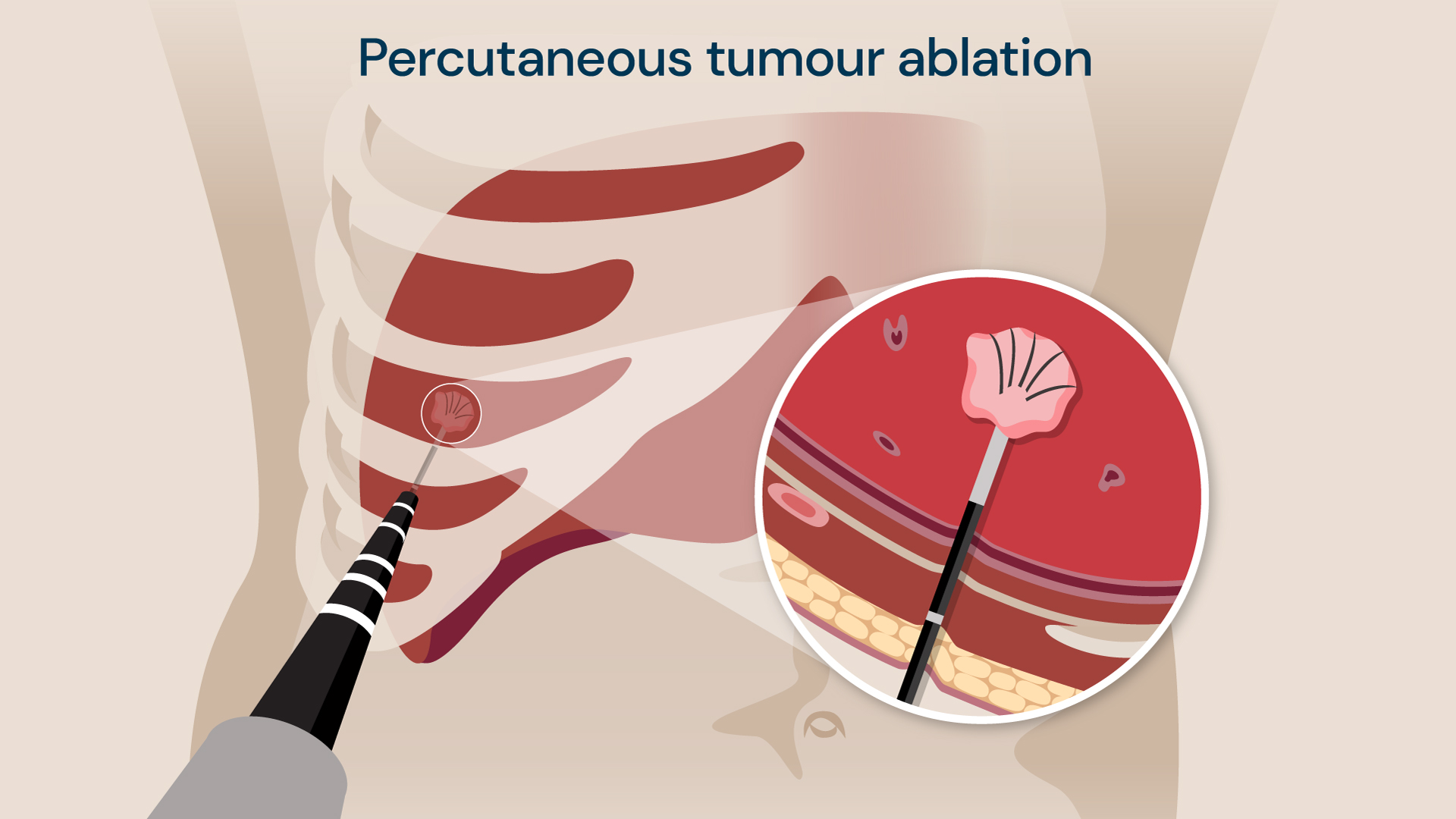
A ‘pinhole’ technique is used by our consultants to deliver hot or freezing treatment to kill the cancer cells in the lung.
Hot (microwave therapy) or freezing (cryotherapy) temperatures are used at the tip of the probe to kill the tumour cells. This procedure is used when the tumour is located outside the airway.
Hot temperatures may be used in deeper lung tissues (where there is a lot of lung tissue surrounding the tumour), while cold temperatures may be used near the delicate outer lining of the lung. This procedure is usually performed with general anaesthetic and takes 1 hour.
We are proud of our local tumour control rate of 93.1% following percutaneous tumour ablation, with 97% of patients experiencing minor or no complications. The local tumour control rate means that cancer has not returned at the site of treatment.
Awake ablation
Our consultants have developed a new technique called ‘awake ablation’ where local anaesthetic is used. The specific area to be treated is numbed rather than you being sedated. This is useful for patients that cannot receive general anaesthetic.
Our awake ablation technique has won the coveted LaingBuisson award in 2022 for improving healthcare outcomes, as it offers patients an option to remove their lung tumour with a minimally invasive technique when this was not previously possible.
Single-port video-assisted thoracoscopic surgery (VATS)
For larger lung tumours, surgery may be needed to remove the part of the lung affected.
This is traditionally performed with an open-chest surgery, where the breastbone is cut to access the tumour. However, not everyone suitable for this procedure, such as if you have other health concerns that make you high risk.
Our consultant thoracic surgeons offer a keyhole surgical procedure to remove lung cancer, called single-port video-assisted thoracoscopic surgery (VATS). This can be offered to patients as a minimally invasive alternative to open chest surgery.
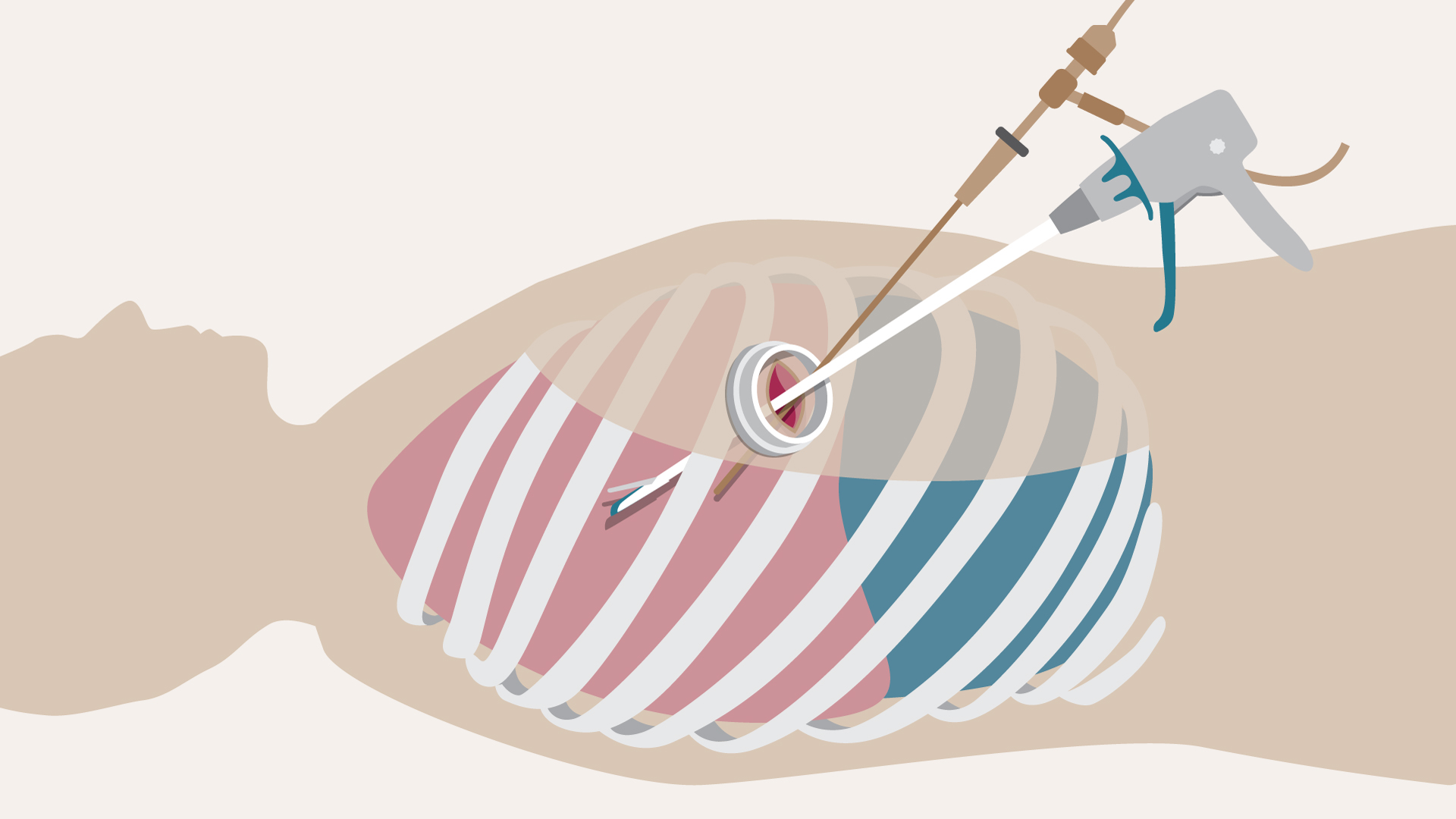
A single-port (also called a single-incision) VATS procedure is a minimally invasive keyhole technique that can be used to remove lung cancers.
A single incision is made in between the ribs (a port) to enable our surgeons to insert a camera and surgical instruments needed for the VATS procedure.
Our consultants were actively involved in the VIOLET study to understand the outcomes of the VATS procedure. The study showed that the VATS procedure resulted in significantly less pain, fewer complications and a faster recovery when compared to open chest surgery.
Robotic-assisted thoracic surgery (RATS)
Robotic-assisted thoracic surgery (RATS) is a type of minimally invasive surgery used to treat conditions inside the chest, including the lungs.
The procedure is performed using the da Vinci Xi robotic system. Our surgeons will make between 3 and 5 small cuts (around 8-12mm in size) in your chest wall and will then insert the robotic arms through these incisions. The robotic arms hold miniature surgical instruments and a 3D camera, providing a detailed view of the inside of your chest wall and lungs.
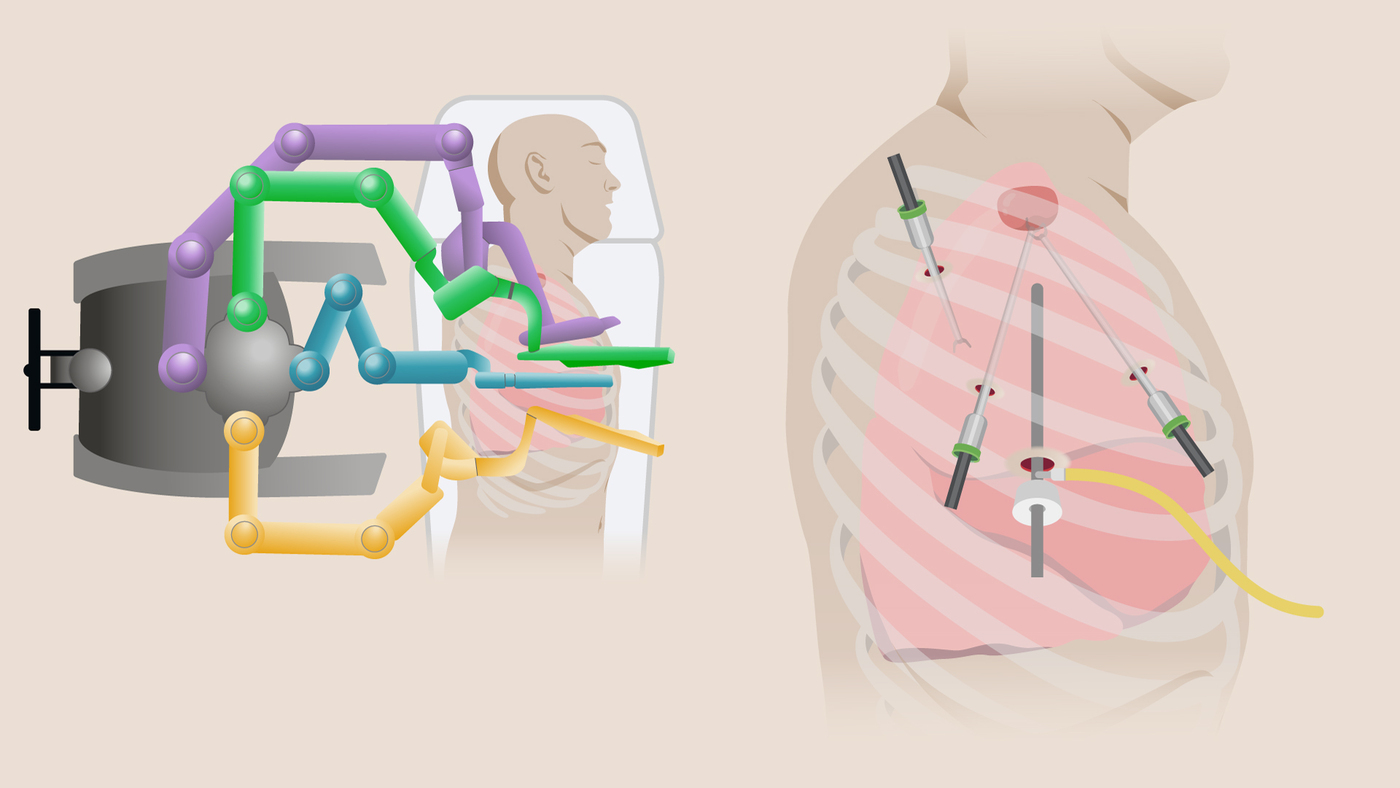
The da Vinci Xi robotic system has 4 arms which are used to perform the minimally invasive thoracic surgery.
The robotic system, using robotic arms entirely controlled by the surgeon, allows for improved precision when removing the lung tumour, less pain and faster recovery times.
Our consultant will assess your condition to decide if RATS is the best treatment option for you. In some cases, another surgical approach – like open surgery or VATS – may be more appropriate.
Day case lobectomy
Lobectomy is the surgical removal of a lobe of the lung. In the case of lung cancer treatment, the procedure is carried out to remove one or more tumours from the affected part of the lung.
Our specialist team can perform lobectomies minimally invasively, with the majority the of operations carried out through a single 3cm incision, through which both a camera and keyhole instruments are inserted. This allows your pain to be far better controlled, allowing you to resume your usual activities sooner with reduced pain.
In some cases, depending on recovery immediately after the procedure, our patients can return home on the same day as their procedure to continue to recover in the comfort of their own home.
Cryotherapy pain relief for chest surgery
The recovery process following open chest surgery and minimally invasive VATS procedures is associated with pain that needs to be managed with medication. Patients can also experience limited movement due to pain that requires physiotherapy to support healing.
Royal Brompton Hospital is the first in the UK to offer cryotherapy treatment that is applied during chest surgery to offer pain relief for up to 6 months post-surgery. It works by temporarily ‘shutting off’ the affected nerves in the chest that transmit pain signals to the brain, numbing the area operated on.
To learn more about options for lung cancer treatment with our specialists, contact our team today.
Related services
-
CT scan
A CT uses X-rays and a computer to produce images of many structures inside the body.
-
Diagnostic tests for lung conditions
Our dedicated specialists diagnose and treat adults and children with a range of conditions at our innovative, ground-breaking heart and lung centre.
-
Hypoxic challenge test
A hypoxic challenge test is used to assess whether you need extra oxygen while travelling on a plane, due to the reduced levels of oxygen in aircraft cabins.
-
Lung cancer risk assessment
Our world-leading specialists can assess your risk of developing lung cancer during a consultation.
-
Lung health assessment
Our lung health assessment service offers a range of diagnostic tests that help us examine your lung health. Learn more about the conditions we test.
-
MRI scan
An MRI scan is a medical imaging technique that uses a magnetic field and radio waves to create pictures of an internal cross-section of the body’s structures.
-
Percutaneous cryotherapy
Percutaneous cryotherapy treatment involves freezing a lung tumour – to kill the cells in it – using a CT scanner for guidance.
-
Tumour ablation for lung cancer
Tumour ablation is a procedure that uses heat or cold treatment to kill a tumour inside the lungs. Find out more about this procedure.
Reviewed regularly to reflect clinical best practice
Last reviewed: 09 March 2026
Locations
Diagnosis and treatment for lung cancer is available at the following locations: