
Content verified by

Our consultant cardiac surgeons, led by Mr Toufan Bahrami, have developed and operated on over 2,000 patients with totally endoscopic (keyhole) procedure to repair the heart’s mitral, tricuspid and aortic valves. This minimally invasive treatment, first performed in the UK at Royal Brompton and Harefield hospitals, offers an alternative to invasive open-heart surgery, allowing for significantly improved patient recovery and less scarring.
Innovating valve repair surgery
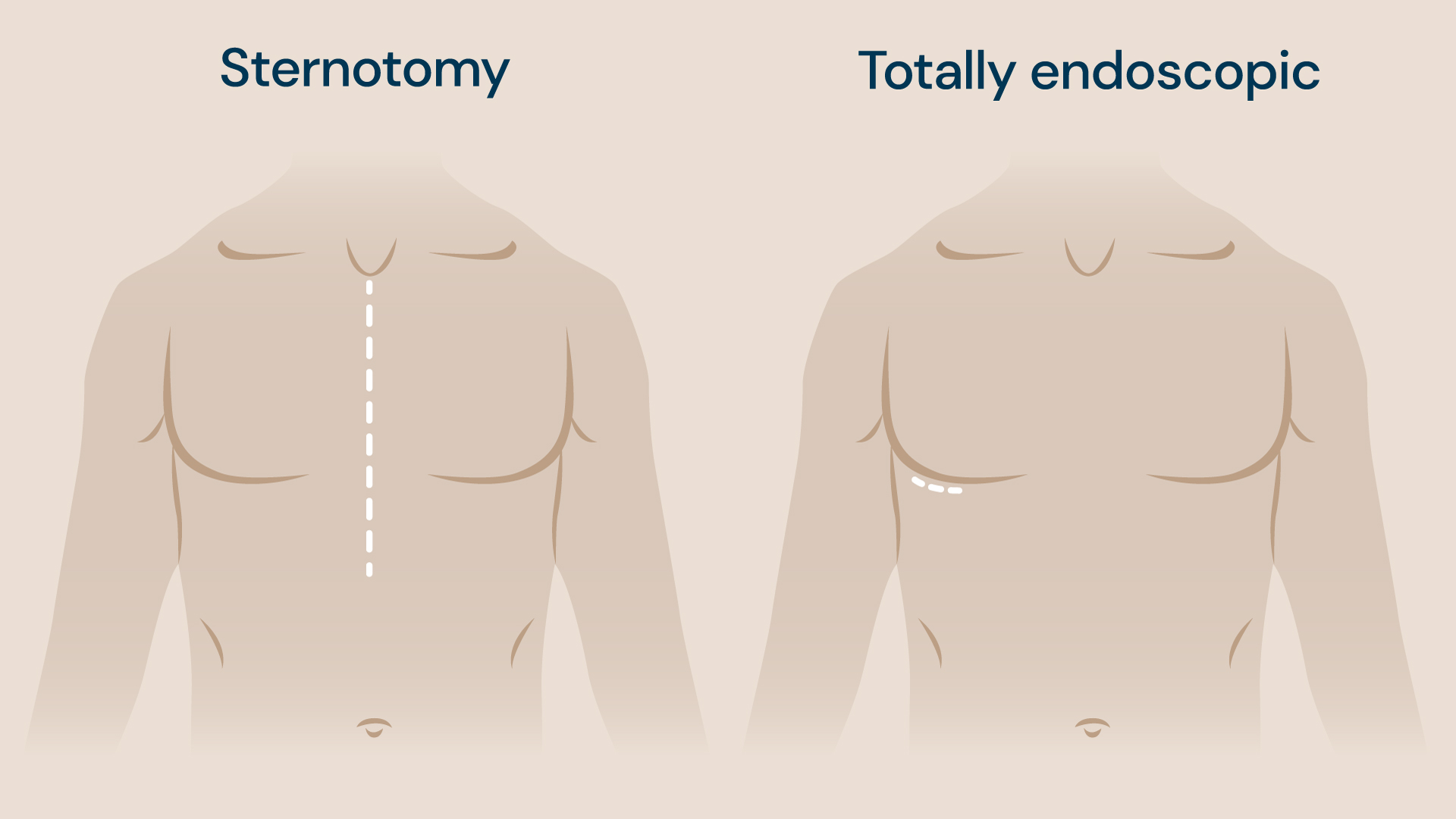
Previously, sternotomy was the well-established procedure for treating mitral, tricuspid and aortic valve disease. This involves making an incision – typically 20-30cm long – over the sternum to access the heart and blood vessels for treatment, before reconnecting the sternum.
However, after making adaptations towards sternotomy with a smaller incision, and then to a minimally invasive procedure, our consultants, led by Mr Toufan Bahrami, have now evolved the treatment into a completely endoscopic procedure performed through an incision of approximately 2.5cm in around 3 hours.

The procedure relies on the use of 3D cameras to project detailed footage of the patient’s heart onto a 3D screen, allowing the surgeon to work by focusing on the screen and not by looking at their hands or directly into the incision. We are the only hospital in the UK to perform this totally endoscopic treatment and we have a dedicated cardiac team for valve repair.
The history of minimally invasive and endoscopic surgery
Driven by the goal of improving patients’ recovery times, reducing their pain levels, and performing a more accurate and precise surgery, Mr Bahrami and his team have led a number of innovations in the field of valve repair surgery over the years. From 2010 to 2015, the procedures they performed were minimally invasive. This involved making a small incision of around 6-7cm in the patient’s side to access the heart valve during surgery.
Following this came endoscopic assisted treatment which was used from 2015 until 2021. In these procedures, the surgical team still looked through the incision, rather than relying entirely on the camera to complete the procedure, but some parts of the operation were endoscopic.
Mr Bahrami and the team then began performing the totally endoscopic procedure in 2021, using camera footage projected onto 3D screens, combined with 3D glasses, to operate instead. They have now performed this endoscopic procedure over 2,000 times, and Mr Bahrami explains, “without minimally invasive and totally endoscopic options, we would not be able to provide these gold-standard results.”
Repair rates in sternotomies vs. endoscopic procedure
To further prove the benefits of endoscopic heart valve surgery, Mr Bahrami’s team participated in a multicentric trial over the last 5 years. The research compared the results of standard sternotomies versus minimal access procedures in mitral valve surgery.
Based on this research, in April 2023, the Journal of the American Medical Association (JAMA) published a study showing that the repair rate is the same across sternotomies and minimal access procedures, including endoscopies. Minimal access surgery is therefore just as safe as sternotomy, but with a significantly improved recovery time.
3D technology in cardiac surgery
Open heart surgery versus keyhole heart surgery
To perform the procedure, a small incision is made between the ribs to insert the endoscope with a camera at the end. The artery and vein are used to perform the bypass, avoiding the need for any major incision. During the endoscopy, a high-definition 3D camera is used to direct the procedure inside the heart through a small incision (2.5cm) in the chest.
Wearing 3D glasses and guided by images projected onto a 3D screen, the surgeon can then repair or replace the damaged valve using specially designed longer instruments. Not only does this technology produce better results for the patient, but it means that every medical staff member in the room is able to see the surgery in detail.
“The projected images can also be accessed remotely via the internet,” adds Mr Bahrami. “This provides a new way for us to combine our multi-disciplinary expertise for the best outcome of care, allowing our specialists to collaborate from anywhere in the world.”
Significantly improved patient recovery
After endoscopic valve repair surgery, patients are usually discharged in around 4 days and are back to their normal activities after 3 weeks. This is significantly faster than the 3-4 months of recovery required after a sternotomy, even though the two types of procedures take a similar amount of time to carry out.
Mr Bahrami explains, “the goal is not to make the operation shorter than a sternotomy – it’s to provide superior surgical repair and a quicker, less painful recovery period.” This comes from eliminating the need for the 20-30cm chest incision made in sternotomies and its associated effects on the respiratory mechanism, as well as reducing postoperative pain. To this end, some of Mr Bahrami’s patients have even been walking 15,000 steps a day and are back to driving within their first 2 weeks of recovery, a level of activity rarely achievable so soon after conventional open-heart surgery.
Committing to training and education
Our pioneering technology and surgical techniques used for endoscopic mitral, tricuspid and aortic valve surgery allow us to demonstrate our commitment to learning and education by providing valuable teaching opportunities worldwide.
Mr Bahrami is currently collaborating with the biomedical engineering group at St Thomas’ Hospital on the development of an artificial intelligence and virtual reality-based training platform for endoscopic surgery.
“We routinely record procedures and integrate the surgical footage with artificial intelligence to create an advanced training programme,” explains Mr Bahrami. “This enables surgeons and trainees to practise endoscopic techniques in a virtual environment before performing them in the operating theatre.”
Medical governing body, The Society of Cardiac Surgeons, recommends that a minimally invasive approach should be the first port of call for all patients. If a patient’s primary surgeon doesn’t perform the treatment, they must be referred to a provider who does. Our commitment to education and training within the medical profession will, in time, make endoscopic surgical options more widely available, benefiting more patients.
Mr Bahrami is a member, and was the president (2024–2026), of the British & Irish Society for Minimally Invasive Cardiac Surgery, where he is actively promoting safety, structured training, and the standardisation of minimally invasive cardiac surgical techniques. These advancements aim to enhance both surgical outcomes and patient recovery on a global scale, working toward establishing minimally invasive valve repair as the standard of care.
Robotic and endoscopic cardiac surgery
Robotic surgery is fundamentally an advanced form of endoscopic surgery. The da Vinci Surgical System is currently not certified for cardiac procedures in Europe and has only recently received approval for cardiac applications in the United States.
Our team has performed more than 2,000 totally endoscopic procedures with outstanding clinical outcomes, and is now at the verge of introducing robotic surgery into our practice. Given that robotic and totally endoscopic techniques share approximately 95% technical similarity, the transition to robotic surgery will be seamless and associated with extremely low risk.
Our extensive expertise in totally endoscopic cardiac surgery uniquely positions us to become one of the safest centres for performing robotic cardiac surgery in the future.
When to refer to us
Patients can be referred to us for repair of the aortic, mitral or tricuspid valves. Our expert team can perform endoscopic valve repair for both stenosis and regurgitation and are proud to be the only providers in the UK of this treatment endoscopically.
Get in touch
Patients can be referred to us for repair of the aortic, mitral or tricuspid valves. Our expert team can perform endoscopic valve repair for both stenosis and regurgitation and are proud to be the only providers in the UK of this treatment endoscopically.
Reviewed regularly to reflect clinical best practice
Last reviewed: 13 March 2026