
Authors

The transcatheter mitral edge-to-edge valve repair (M-TEER) programme at Royal Brompton and Harefield hospitals is one of the most experienced and comprehensive in the world. Dr Robert Smith leads the most experienced M-TEER team in the UK. He has treated more than 1,500 leaky mitral valves with this therapy.
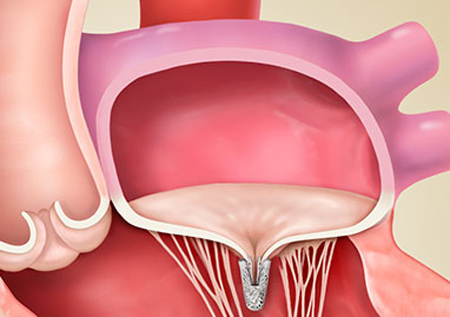
Faulty mitral valves are one of the most common causes of cardiovascular disease (CVD) and can be caused by age-related changes to the heart. Experts at Royal Brompton and Harefield Hospitals have been leading the way in recent years to develop lifesaving alternatives for patients who are at increased risk from conventional open-heart surgery, or who might benefit from a minimally invasive approach. Human heart valves are exceptional structures. The mitral valve is very complex with thin valve leaflets attached to the heart wall via multiple string-like chords. Opening with every heartbeat, millions of times over a lifetime, the valve is susceptible to wear and tear.
What is mitral regurgitation?
As the heart beats, the mitral valve and tricuspid valve control blood flow from the atria to the ventricles. If the mitral valve’s two leaflets do not close effectively then this allows blood to flow backwards at high pressure through the valve into the left atrium.
Known as mitral regurgitation (MR), it causes the heart to work harder to push blood around the body. Mitral regurgitation is often associated with heart failure which is one of the most common cardiovascular disorders worldwide. Patients may experience symptoms such as fatigue, shortness of breath and worsening heart failure. It can also put further pressure on the pulmonary vessels, and in severe cases, this can result in fluid congestion of the lungs.
Mitral regurgitation can be related to age, coronary artery disease, underlying heart muscle disease (cardiomyopathy) or a birth defect.
Treating the leaky valve
Mitral regurgitation can be successfully treated by experts at Royal Brompton and Harefield Hospitals. Conventionally, degenerative mitral regurgitation is treated by open-heart surgery which, in older or frailer patients, can be associated with a higher risk and longer recovery time.
In situations where the risk of surgery is too high, or when the regurgitation is ‘functional’ (i.e. due to a weak heart muscle), open-heart surgery may not be appropriate.
The M-TEER device is a small clip that is attached to the mitral valve. There are currently two commercially available TEER devices used at Royal Brompton and Harefield hospitals: MitraClip™ system (Abbott, US) and the PASCAL Precision system (Edwards, US). These implants treat mitral regurgitation by allowing the mitral valve to close more effectively, helping to restore normal blood flow through the heart.
As a transcatheter procedure, the M-TEER device is a less invasive approach compared to conventional surgery. Using this technique, access to the heart is via a small incision in the groin and the mitral valve is repaired through a catheter inserted via the femoral vein.
Once the catheter is guided to the heart, a small hole is made to enable the catheter to cross from the right to the left side of the heart. The guiding catheter is then steered into the left atrium. This small device is then used to literally ‘clip’ the leaking portions of the valve leaflets together.
During the procedure to fit the device, a radiographer is on hand with an x-ray machine, to provide the images to guide the interventional cardiologist. In addition, another cardiologist guides a transoesophageal echocardiogram (TOE), which uses ultrasound from a probe to check the structure of the heart and how well it is functioning. This allows for real-time mitral regurgitation reduction assessment on the beating heart, and thereby avoids cardiopulmonary bypass.

An example of M-TEER device (MitraClip). The clip is attached to a highly manoeuvrable delivery catheter.
Quick improvement
The procedure usually takes between one and two hours and immediately reduces mitral regurgitation. Patients often feel a change to their quality of life very soon after the procedure.
Recovery is faster than conventional surgery, and patients are usually discharged from hospital after a few days.
Dr Smith adds
“After 48 hours, they have a significant improvement. M-TEER therapy is associated with symptomatic improvement in 90 to 95 per cent of patients. It’s proven to be good at relieving symptoms and can generally be performed at low risk of serious complication.”
“Additionally, a major study – COAPT* – has demonstrated that M-TEER treatment with MitraClip improves survival and reduces hospital admissions for functional mitral regurgitation.”
A whole team of specialists
Dr Smith highlights the benefit of being treated by an experienced multidisciplinary team at Royal Brompton and Harefield hospitals:
“We are a world-leading transcatheter mitral service. As the most experienced UK centre, we have now carried out well over 1,000 cases.
A patient requiring treatment is not just getting me as a consultant – they’re getting a whole team. I work closely in a highly skilled team with surgeons, cardiologists, anaesthetists and nurses.”
Dr Smith’s team are continually pushing the boundaries, in addition to M-TEER, the team are undertaking many new and innovative transcatheter procedures to treat both mitral and tricuspid valve disease. The team now also offer TEER for the tricuspid valve as well as transcatheter mitral and tricuspid valve replacement (TMVR and TTVR).
Reviewed regularly to reflect clinical best practice
Last reviewed: 01 July 2026
See also
-
Coronary heart disease
Coronary heart disease is caused by the narrowing of the coronary arteries that supply the heart muscle with oxygen-rich blood.
-
Heart valve repair or replacement
Heart valve surgery can repair or replace a damaged valve.
-
Mitral regurgitation
Mitral regurgitation is the most common heart valve problem worldwide. It is a dysfunction of the heart’s mitral valve.
-
Mitral valve repair and replacement
Mitral valve repair and replacement surgeries are used to fix problems with your mitral valve. Discover more about these surgeries.
-
Thoracic endovascular aortic repair (TEVAR) procedure
TEVAR uses a stent-graft to reinforce and repair a weakened section of the aorta.
-
Valvular heart disease
Heart valve disease occurs when the valves of the heart become diseased or damaged.