
Content verified by

One-stop diagnostic service for childhood colorectal disorders
Young patients with chronic constipation or faecal incontinence may suffer from severe discomfort and psychological issues. Accurately diagnosing which colorectal disorder a patient has is key to developing the best treatment plan. Our specialists at Evelina London Children’s Hospital have developed a one-stop diagnostic service for colorectal disorders including anorectal manometry, endosonography and colonic transit. Mr Ali Keshtgar, consultant paediatric colorectal and neonatal surgeon, explains more.
Establishing the cause of chronic constipation and faecal incontinence
Childhood constipation is common, affecting 10-20% of children in the UK. Approximately 30% of children aged 4-11 years old have symptoms of constipation lasting less than 6 months, and 5% may have constipation lasting longer.
Most children develop constipation at the time of toilet training around 2-3 years of age. They may experience painful passage of stool and develop a vicious cycle of withholding behaviour and retention of stool in the rectum, which becomes harder, larger and more difficult to pass. Most children respond to early medical treatments such as laxatives, toilet training and dietary modification, while other patients may also benefit from psychological support.
However, for some children, medical treatments do not work and constipation may become chronic, leading to faecal incontinence and the development of a large size rectum, which is more difficult to treat. This can occur for several reasons, including inappropriate contraction of the voluntary muscles of external anal sphincters (EAS) because of fear of defecation and withholding behaviour.
Other children may have Hirschsprung’s disease in which the automatic muscles of lower bowel and involuntary muscles of internal anal sphincter (IAS) do not relax properly. This problem mainly affects babies but, in rare cases, our specialists see it in children who have had trouble passing stools since they were babies. These children do not get better by taking medicine alone and often require surgical intervention.
One-stop 3D investigative package and treatment
“We have developed a one-stop service of anorectal manometry, endosonography and colonic transit study to investigate constipation and faecal incontinence in children,” says Mr Keshtgar. “We can also offer the treatment of botulinum toxin for functional constipation as a day case admission, which is unique in London, and we’re one of only a few centres in Europe to offer this.”
For children with defecation disorders, our one-stop service of highly specialised investigations includes:
- 3D high resolution anorectal manometry
- anal endosonography
- colonic transit study
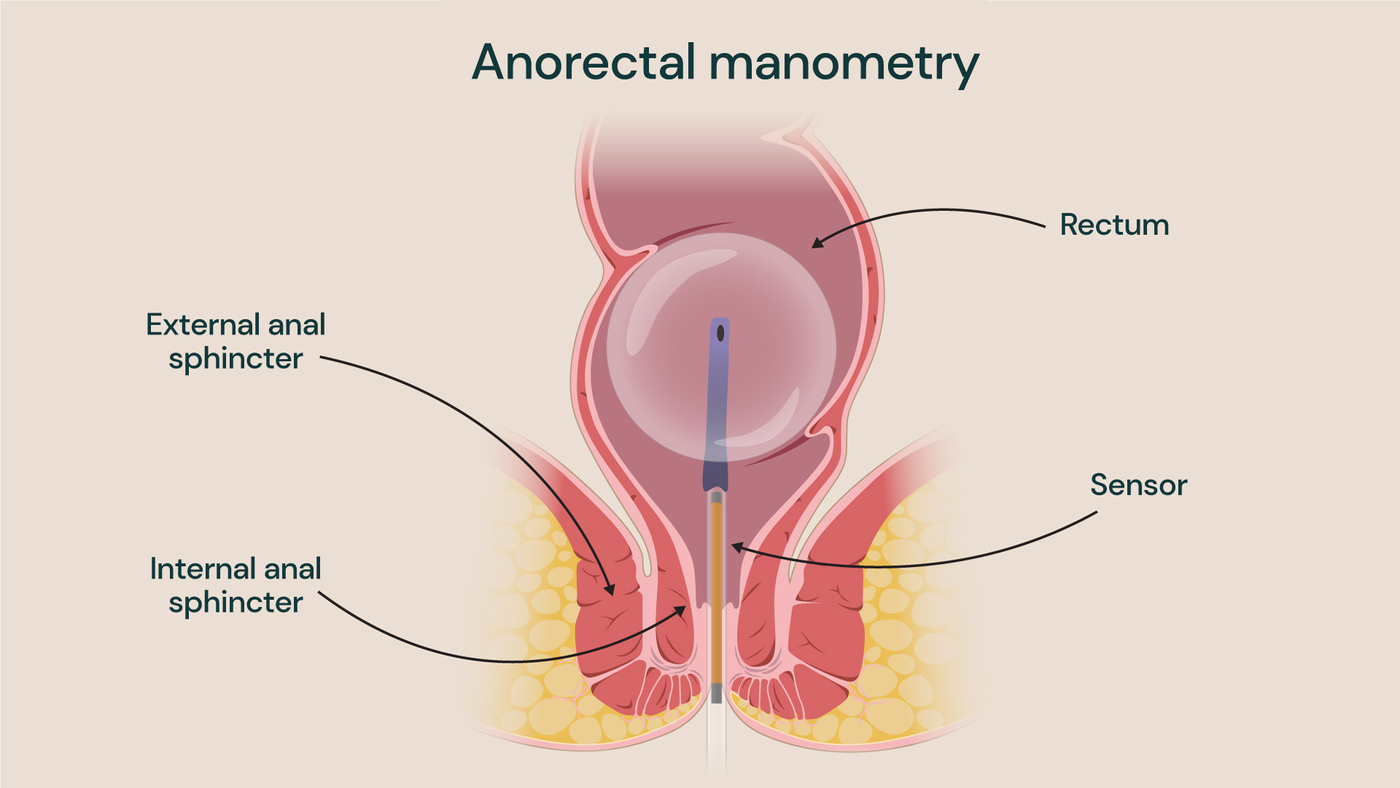
Our paediatric surgeons and gastroenterologists use the latest 3D high resolution anorectal manometry, which measures how effectively the muscles and nerves of the gastrointestinal system function.
The anorectal manometry begins with inserting a small tube with a balloon on the end while the patient is sedated. To assess the patient’s rectal anal inhibitory reflex (RAIR), the balloon is inflated in the rectum, which determines how strong the muscles around the back passage are. This provides functional information about the relaxation of the anal sphincter and the lower part of the bowel. Our specialists then check how well the sphincter is working and if there is any information about the cause of constipation or incontinence there.
Previously, this information could only have been collected by taking a rectal biopsy, which comes with risk of infection and bleeding, and does not always generate an accurate specimen. In unsuccessful cases, the rectal biopsy may have to be repeated in another procedure, which is more invasive and does not provide the functional information that the high resolution anorectal manometry does.
“The anorectal manometry, combined with the endosonography (to show the structural morphology of the lower part of the rectum), as well as the colonic transit study, gives us the full picture of what’s going on,” explains Mr Keshtgar. “This enables us to offer appropriate, timely treatment to our patients in a one-stop day admission.”
Combining investigations and treatment
As a result of Mr Keshtgar’s pioneering research work at Evelina London, Guy’s and St Thomas’ hospitals, he introduced botulinum toxin (botox) as a new treatment modality for chronic functional constipation and soiling in children, which is now used worldwide. He explains, “a single injection of botox into the external anal sphincter is effective in about 80% of children and about 10% of patients may require a second injection to treat their condition.”
If the investigative procedures show that the botox injection would be beneficial to the patient, it can be administered while the patient is sedated, with the patient returning home on the same day. In rare cases where the investigative procedures demonstrate that botulinum toxin treatment would not be sufficient, our specialists have the surgical expertise to offer a range of treatment options. This includes formation of an antegrade colonic enema (ACE) stoma, in which the appendix is used to make a small hole on the lower abdomen to pass a catheter for colonic irrigation.
Multidisciplinary teams (MDT) for a unified approach
Mr Keshtgar has set up an MDT approach for complex patients with regular input from gastroenterologists, child psychologists, urologists and bladder and clinical nurse specialists. Opening up this new communication channel ensures a unified approach between teams, as well as benefitting ongoing research in multiple specialties.
“Regular MDT meetings are another way of offering the best expert opinions and service, and also allow us prevent duplication of appointments for our patients,” explains Mr Keshtgar. “Additionally, our MDT approach is a type of safeguarding, ensuring that our young patients are not subjected to any unnecessary operations or treatment.”
Seamless transition to adult services
Over the last 5 years, Mr Keshtgar has worked to establish a new service to aid the transition of his adolescent patients to care under an adult colorectal surgeon. Many patients need long-term follow-up care and surgical input, so Mr Keshtgar and his colleagues at Evelina London work to prepare them for a successful transfer to specialist colorectal colleagues at St Thomas’ Hospital.
Evelina London and St Thomas’ facilities are adjoined, providing a very smooth journey for our young patients from the ages 14 to 16. The transition process takes place over 1-2 years to ease the transfer process for patients and their families from paediatric to adult care. This is included as part of our colorectal care packages at Evelina London.
When to refer to us
At Evelina London, we are proud to offer this one-stop service, utilising equipment which is not widely available amongst other private hospitals or NHS trusts. With the recent opening of our purpose-built Children’s Day Surgery Unit at Evelina London, we are pleased to accommodate more private patient referrals.
Patients can be referred to us for investigations and surgical treatments for their constipation and faecal incontinence if previous medical treatments under the care of paediatricians and gastroenterologists have failed. This is to safeguard our young patients from any unnecessary surgical intervention, and to ensure that all other medical treatment options have been exhausted first.
Mr Alireza Keshtgar
Mr Ali Keshtgar specialises in paediatric colorectal surgery, including operations on newborns, general and minimally invasive keyhole surgery in children.
He introduced the new treatment of botulinum toxin injection into anal sphincters for childhood constipation as part of his PhD research project, which is now used worldwide.
Get in touch
To find out more about our colorectal manometry service and our investigations and treatment for childhood chronic constipation, please contact our customer service team.
Call 020 3131 5130 or email privatepatientenquiries@gstt.nhs.uk.
Related content
-
Anorectal manometry, endosonography and colonic transit study in children
Anorectal and colonic studies include a set of tests carried out to establish the causes of constipation and faecal incontinence. Learn more about our expertise.
-
Children's gastrointestinal surgery
Our paediatric gastrointestinal surgeons specialise in upper, lower and colorectal treatments as well as general children's surgery.